Empathy helps healthcare providers to create a positive interpersonal relationship that creates a non-defensive environment, and allows the patient to be more forthcoming (Mercer and Reynold, 2002; Hemmerdinger et al, 2007; Neumann et al, 2011; Petrucci et al, 2016). Empathy is an important characteristic in the relationship between a healthcare practitioner and his or her patients. When empathy is present, it can enhance both the patient and the provider's overall experience. There are different understandings of the word empathy and what being empathetic is; the general consensus of the definition states that empathy is the understanding of another person's reactions, thoughts, feelings and problems (Eisenberg, 2000; Myers, 2000; Burks and Kobus, 2012, Petrucci et al, 2016). Empathy involves not only understanding another person, but demonstrating that understanding back to the patient while maintaining emotional detachment (Burks and Kobus, 2012). The ability to communicate this understanding and a paramedic's intention to help is important to create an environment that is empathetic and open (Petrucci et al, 2016).
There is an important need to differentiate empathy from sympathy in health care, as failing to do so could lead to misdirection in patient support. Sympathy is an expression of concern or sorrow about stressful events in a person's life; this expression usually comes from judgement and may not be in the interest of the patient (Meier and Davis, 2008; Clark, 2010). Sympathy may also prove ineffective when a paramedic assumes that his or her own experience matches or equates to that of the patient (Egan, 2010). Not only is expressing sympathy a disadvantage to the patient and their care, it is also a disadvantage to the paramedic. If healthcare providers assume the emotional burden of every patient they encounter, it may not take long before they begin to suffer compassion fatigue and burnout (Hamilton et al, 2016; Williams et al, 2017). Therefore, it is imperative to know the difference between empathy and sympathy, and how to demonstrate the appropriate trait during patient interactions.

Clinical outcomes have been shown to improve when patients perceive their healthcare provider to be empathetic (Burks and Kobus, 2012). This open climate encourages patients to be more vocal about their symptoms and problems, allowing health providers to obtain more accurate information, and facilitates better overall clinical care (Burks and Kobus, 2012). There are many favourable outcomes for patients when empathy is demonstrated; examples include reduced psychological stress, improved self-concept, reduced rates of anxiety and depression, and lower complication rates (Reynolds, 2000; Hojat et al, 2011; Canale et al, 2012). The ability to set one's emotions aside when practising empathy can be particularly beneficial to the provider in terms of preserving their professional wellbeing and positively influencing clinical encounters (Burks and Kobus, 2012).
Previous studies of healthcare students in Australia (McKenna et al, 2012; Williams et al, 2012; 2014; 2016) have demonstrated that empathy scores are low among paramedic students; scores decrease as one progresses through paramedic education; and empathy scores vary significantly for certain medical conditions.
Aim of the current study
The aim of the current study was to assess empathy scores of first and second year paramedic students at Fanshawe College in Ontario, Canada. The authors hypothesised that in concordance with existing evidence, empathy scores would vary across medical conditions, and that certain medical conditions would elicit lower empathy scores.
Methods and materials
This study was cross-sectional, using a web-based questionnaire and convenience sampling of first and second year paramedic students at Fanshawe College in Ontario, Canada. Ethics approval was granted by the Research Ethics Board at Fanshawe College (approval S16-00-1).
The Medical Condition Regard Scale (MCRS) and demographic questions were input into Google Forms, and a link to anonymously complete the form was provided to participants. An invitation to participate was distributed via a closed social media group consisting only of paramedic students. Participants were provided with an explanatory statement and informed that participation was voluntary and anonymous.
This study used the MCRS, a 6-point Likert scale consisting of eleven statements for each medical condition. The MCRS is a validated tool used to measure empathy, regard, and bias for a number of medical conditions (Christison et al, 2002). The MCRS has a Cronbach-α coefficient of 0.87 when assessed for internal consistency and a test-retest reliability coefficient of 0.84 (Christison et al, 2002). The statements in the MCRS investigate common stigmas, likes, dislikes, and the desire to treat patients with certain medical conditions. This scale has previously been used to measure empathy levels in medical and nursing students, as well as in paramedic students (McKenna et al, 2012; Williams et al, 2012; 2016). Other scales exist to measure empathy, such as the Jefferson Scale of Empathy. The authors of the current study elected to use the MCRS owing to its simplicity, ease of use, proven validity and consistency; and to allow for comparisons to previous studies of other healthcare professions students that also used the MCRS.
The MCRS requires respondents to rate their agreement to each statement from 1 (strongly disagree) to 6 (strongly agree). Five questions are phrased negatively and thus the scores for these questions are reversed for analysis (strong agreement with these questions would indicate lower empathy). Overall empathy scores can vary from the lowest score (55) to the highest score (330). For each individual medical condition, scores can vary from the lowest score (11) to the highest score (66). Higher scores indicate a higher regard of empathy for the medical condition in question.
The present study used the MCRS to assess empathy levels for five medical conditions:
These conditions were selected based on previous studies of empathy levels in healthcare professions. In addition to the MCRS, brief demographic questions were posed regarding age, gender, year of study in the paramedic programme, and open-ended questions investigating students' perceptions on empathy education in the programme.
The Statistical Package for Social Sciences (SPSS; v. 20.0, New York USA) was used for data storage, tabulation and the generation of descriptive statistics. Means, t-tests and one-way analysis of variance tests were used to assess differences between age groups, gender, and year of study. Results were considered statistically significant if the p-value was less than 0.05.
Results
A total of 43 paramedic students participated out of a possible 90 (47.8% response rate). Respondents comprised 18 (38.3%) first year students and 25 (61.7%) second year students, with 15 females (35.7%) and 27 males (64.3%). One respondent did not respond to the gender question. Male paramedic students displayed a mean empathy score of 232.44 (standard deviation (SD) ±29.17), while their female counterparts had a statistically significant higher mean score of 266.4 (SD±29.99) (p=0.001)
There was notable variance between respondents' attitudes towards patients with the five different medical conditions as measured by the MCRS. Physical disability and intellectual disability were held in similar regard according to the MCRS. Suicide attempt and mental health emergencies were held in lower regard, with substance abuse held in significantly lower regard by respondents. Means for each medical condition are presented in Table 1.
| Medical condition | Mean | SD |
|---|---|---|
| Intellectual disability | 50.42 | 8.73 |
| Physical disability | 53.00 | 7.22 |
| Suicide attempt | 49.47 | 7.75 |
| Substance abuse | 42.88 | 10.62 |
| Mental health emergency | 49.58 | 10.02 |
The respondents were divided into four age groups for analysis. The mean empathy scores between age groups were not statistically significant [F(3, 38)=2.329, p=0.09], suggesting that age does not play a significant role in influencing empathy scores in this population. One respondent did not respond to the age question. There were several statistically significant differences for year of study and gender for mean scores across the five medical conditions. First year paramedic students had a mean empathy score of 257.11 (SD±32.46), while second year students had a mean score of 236.88 (SD±32.10) (p=0.049). First year paramedic students also demonstrated a higher mean empathy score towards mental health emergencies (mean 53.72 v 46.6; p=0.02).
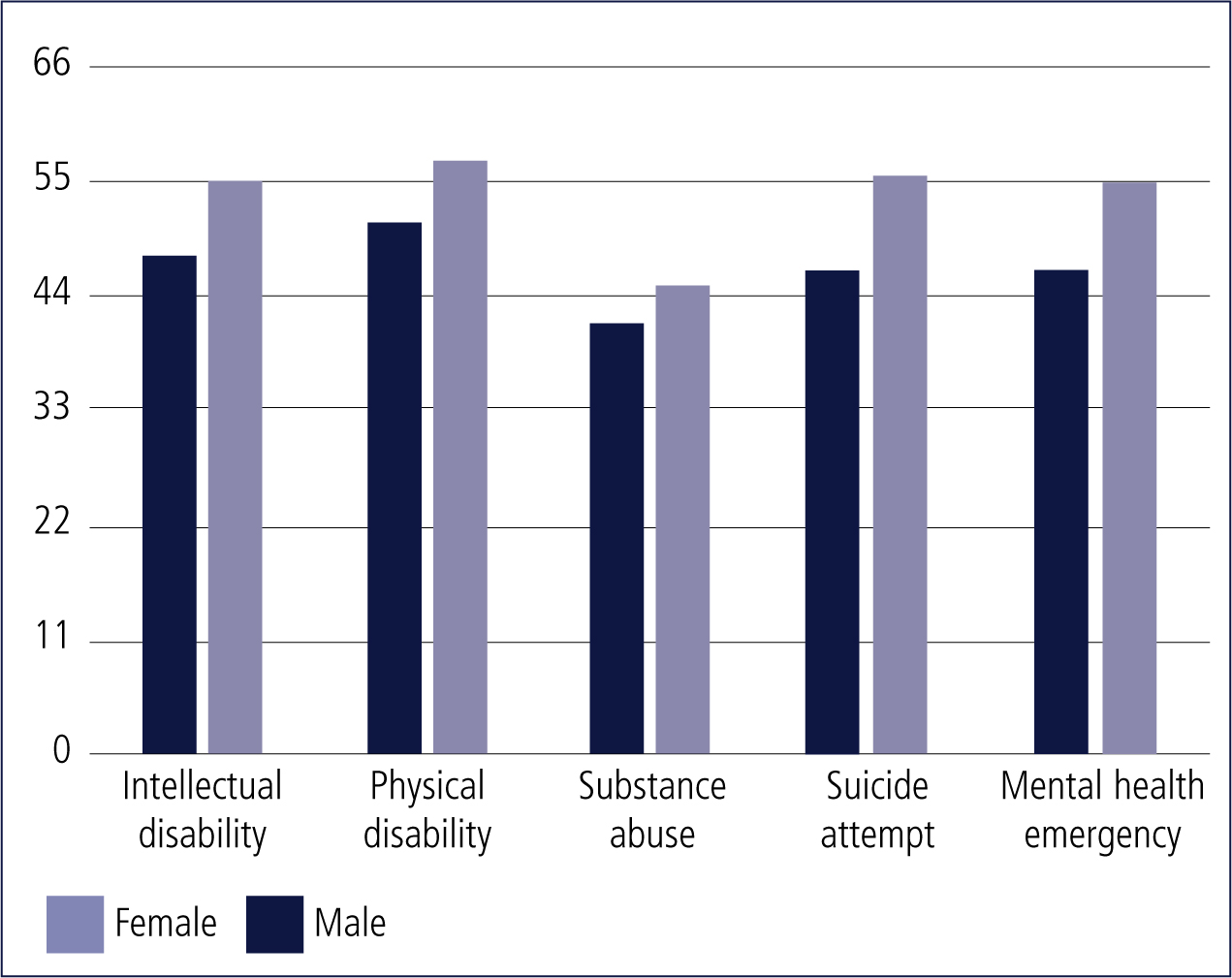
Female paramedic students displayed higher mean empathy scores than their male counterparts for all conditions: intellectual disability (mean 55.0 v 47.66; p=0.008), physical disability (56.66 v 50.81; p=0.011), substance abuse (44.93 v 41.22; p=0.278), suicide attempt (54.53 v 46.44; p=0.001), and mental health emergencies (55.26 v 46.29; p=0.005) (Figure 1).
A total of 37 respondents (86%) indicated that more empathy training was required in the programme. Suggestions to improve empathy training included increasing high-fidelity simulation, inviting guest speakers, and undertaking more mental health service placements. A selection of free-text quotes from respondents, of interest to the research question, were selected:
‘…include holistic/biopsychosocial views of health…’
‘…LTC [long-term care] placements only made people feel less empathy for the elderly patients…’
‘…you can't teach empathy…’
Discussion
The current study demonstrated that empathy scores vary across medical conditions, and are significantly lower when dealing with substance abuse presentations. The results also demonstrate that females display higher empathy scores than their male counterparts, and this is consistent with previous literature (Hojat et al, 2004; Williams et al, 2012; 2015). Our results did not demonstrate any significant differences in empathy scores among age groups, although this is likely attributable to the small sample size.
The low levels of empathy demonstrated for substance abuse could be attributed to the view that substance abuse is a disorder that the patient is responsible for. The stigma around substance abuse creates a belief that the user has the ability to stop using drugs or alcohol whenever they choose to do so. There is a need for further exploration and explanation as to why this disorder is treated with less empathy.
Looi (2008) attributes the differences in male and female empathy scores to differences in brain architecture and neural circuitry. Looi suggests that men are predisposed to being unemotional in order to facilitate more rational decision-making. Regarding differences in empathy with age, Beadle et al (2015) demonstrated that in contexts relevant to socio-emotional goals, adults over the age of 24 may be more motivated than younger adults to help others. They demonstrated this by playing a game (the dictator game) and assessing mood throughout. While the present study demonstrated no differences among age groups, previous studies have revealed differences, with higher empathy scores in middle-aged participants (Williams et al, 2012; 2014).
Differences in empathy scores between first and second year students were also observable in the current study. This trend has previously been demonstrated in nurses, paramedics, physicians, and dentists (Hojat et al, 2004, Nunes et al, 2011, Williams et al, 2012). Studies have found personal distress to be a main cause of empathy decline; other causes are cognitive overload, lack of personability, the modern medical system, and elitist thinking (Paro et al, 2014).
Self-distress was identified as a main cause of empathy decline by Neumann et al (2011) and Williams et al (2012). The most mentioned causes of distress were burnout, low sense of wellbeing, and depression. Vulnerability of students was also a factor related to increased distress. Students have values of idealism, enthusiasm and humanity present at the beginning of their schooling but these diminish as students are confronted with reality during clinical placements. Students showed a decline in empathy and an increase in cynicism when they had late exposure to clinical settings. Possible explanations for this include a student's inaccurate perception of the realities of the job due to misinformation and underexposure. Social support problems arise for students and health professionals who have heavy workloads and work long hours. These students and professionals suffer from reduced contact with their families and a lack of social support from their peers and friends.
Empathy is also shown to decline as education progresses and this is thought to occur as a result of emotional exhaustion, depersonalisation and academic overload (Paro et al, 2014). The large amount of theoretical learning throughout the years overwhelms and distracts the individual from being empathetic. As education progresses, the workload increases and this inevitably causes a decrease in time for self-reflection to maintain empathy.
When studying to become a health professional, education is the main focus. Modern medical education focuses strongly on the scientific aspects rather than the social aspects. Social science and humanistic curriculum is key to developing appropriate bedside manner and an empathetic personality. The strong science focus and the heavy workload does not allow much time for students to incorporate the social aspect of patient interaction. Other reasons outlined in the literature linked to decrease in empathy levels are inadequate role models, elitist thinking and certain personality traits.
Elitist thinking is when a person believes they belong to an elite and privileged group. This thought process may induce a distancing from the patient, which may also be seen as lacking in empathy. Regarding role models, students will inherently model and develop their own empathy and patient care skills from the professionals they work with. Positive role-modelling of empathetic behaviours may help to influence empathy levels among students.
The results of the present study suggest that paramedic students may benefit from focused empathy education and training. Students have mixed ideas (as is apparent in the free-text quotes on the previous page) regarding the training required to understand and improve empathy towards patients, but they do identify a need.
Incorporating focused empathy education may help contribute to a standard level of care for patients and ensure the longevity of the healthcare practitioner's career, as well as create more positive patient-practitioner interactions. There are many recommended methods to increase empathy levels in students and working professionals. These methods include mindfulness training, self-reflection, emotional labour training, and the use of positive role models (Batt-Rawden et al, 2013). Integration of empathy training into the paramedic curriculum could prove beneficial, although the exact type of education, duration, delivery method and curriculum warrants further research.
Limitations
The use of convenience sampling and recruitment via social media, although simpler recruitment methods, mean that results may not be representative of paramedic students across the programme at Fanshawe College, or the province of Ontario. The sample size of 43 also results in a large margin of error in the results of the present study and future studies should aim to enrol larger sample sizes to reduce this margin. There are no data on those students who declined to participate. Those who did participate may have been more attuned to the study's purpose and felt obligated to participate. Respondents may also have participated more than once, as the survey was anonymous. An unknown number of second year students observed a preliminary presentation before responding to the survey, which may have influenced their participation. The MCRS is a self-reported questionnaire that, while providing reliable data, does not account for participants' self-reporting bias. There may be variances between what participants reported, and how they actually conduct themselves in practice.
Conclusion
Findings of the current study suggest that empathy is not demonstrated equally across medical conditions; that it varies by gender and year of study; and that it is likely to decrease as one progresses through paramedic education (as demonstrated in differences between first and second year scores, though we did not study this longitudinally).
Further research needs to be undertaken, with longitudinal studies of empathy levels among paramedic students in Canada. In addition, studying working paramedics longitudinally would offer an insight into the degree of change in empathy over one's career and, furthermore, allow research into reasons for such decline. The topic of empathy in paramedicine opens the door to a plethora of potential research.
Empathy is an important element in a practitioner-patient relationship and, when present, can enhance both the patient and the practitioner's overall experience during an encounter. Further research is required in the clinical environment on this topic. This may help students, faculty members and institutions to view the concept of empathy not as a ‘soft science’ or a ‘touchy-feely’ idea, but rather as a scientific concept with demonstrated clinical, personal and professional benefits.
There is a general lack of formal empathy education in healthcare curricula (Pedersen, 2010; Mishra, 2015) and, as a result—one can speculate—the paramedic profession. The results of the present study suggest that action needs to be taken to improve empathy levels among paramedic students. Further research is required to determine exactly what this action is, and how to best incorporate it into curricula. Acting now to improve empathy levels among paramedic students may result in increased job satisfaction, resilience to compassion fatigue, and improved patient care.